Did you know that in the UK over 50% of people aged 50 and over have diverticular disease? In fact, it’s even more prevalent in the elderly with over 70% of those over the age of 80 suffering with the condition. So why is it that this condition is so common and yet there are a huge number of people who have never even heard of it?
Well, to begin with, in the overwhelming majority of cases, diverticular disease is asymptomatic meaning that it shows no symptoms at all. However, this means that an unlucky minority who suffer from complications of the condition such as frequent pain, episodes of diverticulitis and even the occurrence of perforations and abscesses may struggle to get adequate sympathy from their family and friends and even from their own doctor.
The standard advice in the UK upon diagnosing diverticular disease from a colonoscopy is to eat a diet high in fibre and stay hydrated. While not bad advice for many people, it certainly doesn’t suit everyone. There isn’t a ‘one size fits all solution’ unfortunately since the understanding of the condition even by the medical community is still somewhat limited. Sadly, this can make some sufferers feel alone which is partly why I felt the need to create this blog. But even more valuable than articles and blog posts is the advice and support of others who know exactly what you’re going through.
Remember that you are absolutely not alone while suffering with diverticular disease or diverticulitis and joining an online support group could provide you with the reassurance that you need when you’re feeling unwell or frightened.
If you’re a UK resident or you are a British expat living abroad, consider joining this group of over 4,500 members and a knowledgeable and supportive admin team. You can join by simply clicking the button below which will take you to the Diverticular Disease and Diverticulitis UK Support Group on Facebook. From there, you need to request to join the group and answer the entry questions which are in place to protect the group from spammers and bots.
Do you ever get a burning sensation in your throat or chest? If you do, it’s likely that you are suffering from acid reflux. People may also refer to acid reflux as ‘heartburn’ or ‘indigestion’.
So what is acid reflux? Well, in our stomach, there is a very strong acid. This acid is important for killing bad bacteria and for helping us to break down our food as a part of digestion. The stomach has a special lining to prevent this acid from damaging the walls of the stomach. However, if the acid happens to leave the stomach and move up the oesophagus (US: esophagus) then we may feel the acid burning in our throat or chest.
What are the symptoms of acid reflux?
There are a number of symptoms that people experience. For example, some people get a burning in their throat or chest, other get quite bad chest pains. Acid reflux can even wake us up in the night. In fact, a lot of sufferers find the symptoms of acid reflux worse when they lay down. Some people also experience nausea or a bitter taste in their mouth due to acid reflux
What are the causes of acid reflux?
There are many causes of acid reflux and so this list is not exhaustive, but here are a few of the most common causes.
Overindulgence – eating too much or food that is too rich in fat or sugar can cause acid reflux.
Poor eating habits – eating too large an amount, eating large bites without sufficient chewing, Eating too quickly, swallowing air while eating, eating too late at night. Find out more, here.
Too many antacids – taking too many antacids can make acid reflux even worse by over neutralizing stomach acid
Upset stomach – stomach bugs or eating something that doesn’t agree with us can cause reflux
Overproduction of acid – The overproduction of acid can mean that it travels up the oesophagus
Gastritis – inflammation of the stomach can mean that it produces excess acid or travels up the
Hiatus hernia – this may prevent food passing properly and can make it more difficult for acid to stay down in the stomach
Diseases of the digestive system – For reasons not always understood, bowel conditions such as Diverticular Disease and inflammatory bowel diseases (IBDs) such as Crohn’s and Ulcerative colitis can be linked to acid reflux.
Gallbladder problems or removal – Dysfunction or removal of the gallbladder can cause excess bile which can lead to acid reflux. If you have severe reflux immediately after gallbladder removal, speak with the surgeon.
IBS – Irritable bowel syndrome can affect the transit of food and cause cramping which may lead to acid reflux.
Stomach/Gastric ulcer – stomach ulcers can cause excess acid production
H. Pylori infection – A overgrowth of a bacteria called H. Pylori in the stomach can lead to poor digestion and acid reflux as a result.
Antibiotics/Certain medications – Antibiotics often kill both bad and good bacteria and so a lack of good bacteria that aid digestion can cause some acid reflux, also, some other medications may affect digestion or stomach acid production
Obesity – the excess pressure on the body caused by excess weight can make acid travel up into the oesophagus, causing reflux.
Gastroparesis/Delayed gastric emptying – acid reflux can occur when food stays in the stomach for too long.
Stress/Anxiety – digestion slows down when we experience stress and anxiety, because of this, food tends to stick around in the stomach a little longer and so we can experience acid reflux.
Bariatric surgery – weight loss surgeries can increase the chance of reflux due to the tiny size of the stomach pouch. If this happens, you need to speak with your surgeon to find a solution; this may include medication or further surgery.
How can I prevent acid reflux?
Good eating habits – adopting good eating habits will help prevent reflux. This means eating small meals, taking small bites, chewing well and eating slowly. It also involves not eating late at night. You can read my post on good digestion habitsto find out more.
Avoiding acidic foods – fruit juices, tomatoes, citrus fruits, alcohol, vinegar, coffee are all acidic foods that we eat. Some people can stop their reflux by simple cutting down on acidic foods or removing them from their diet.
Avoiding trigger foods – Some people are triggered by different foods, common triggers may involve nuts, cheese, carbonated drinks, etc. By using a food and symptom diary to identify trigger foods, you can cut these out of your diet.
Avoid smoking and alcohol – smoking and drinking alcohol are both thought to increase the chance of acid reflux since they are both harsh on the stomach. Smoking can also increase the chances of stomach ulcers, so if you suffer with reflux, it’s a good idea to try to quit.
Avoid taking a lot of painkillers unless told to by your doctor – taking too many painkillers can lead to stomach ulcers and excess acid production
Make sure when taking medications to follow the instructions (such as taking with food) – taking medicine on an empty stomach can be bad for the stomach, so be sure to
Avoid stressful situations – Trying our best to not get too stressed out or anxious can help prevent acid reflux.
How can I treat acid reflux?
If this is just a one-off episode of acid reflux, you can take a simple over the counter medication such as an antacid. Branded examples include Gaviscon, Pepto-Bismol, Rennie and Zantac (ranitidine). Take the lowest recommended dose and give it some time to work. This is important because if you take too much of these medicines, they can actually make the reflux worse by causing your stomach to produce even more acid.
If you are experiencing reflux regularly, have a look at if there is something specific that you are eating or doing to cause it. For example, does it only happen after a glass of wine? Or perhaps it happens after you eat tomatoes or drink coffee… The best way to investigate this is to keep a food and symptom diary, you can download a tracker from here. If you do find a trigger, consider cutting this out of your diet.
Sometimes alcohol triggers acid reflux – in some cases it’s best to just avoid it completely…
If you can’t find a specific trigger but you’re a smoker, consider quitting smoking to see if it makes a difference.
Now, if the acid reflux is happens regularly and you are unable to find relief by changing your diets or habits, then it is time to visit your doctor. Be sure to tell the doctor about any other symptoms you are experiencing, for example, abdominal pains or cramps, a change in bowel habits, nausea or vomiting, excessive belching/burping or passing gas and any disruptions to your sleep. If you have been keeping a food and symptom diary, take this along to your appointment. It will really help the doctor to understand your symptoms and provide an accurate diagnosis.
Your doctor may prescribe you a medication to take regularly in order to reduce the amount of acid your stomach produces such as ppis (proton pump inhibitors) such as Omeprazole. However, it is important to find the cause of the reflux rather than only treating the symptoms. To diagnose problems, a doctor may suggest you take a breath test for H. Pylori (a bacteria that can survive in the stomach’s acidic conditions) or undergo an endoscopy/gastroscopy where a camera inserted into the stomach. This allows a doctor to identify problems such as ulcers or inflammation. They can also take tissue biopsies during the endoscopy to test for further problems.
Why you shouldn’t ignore acid reflux…
If you get acid reflux regularly, it’s very important to not ignore it and make sure to get it treated because long-term acid reflux can cause bigger problems. For example, regular acid reflux can cause tooth decay/and tooth acid erosion. It can also cause stomach ulcers, and can even increase your risk of stomach and oesophageal (US: esophageal) cancer in the future.
Do you suffer with acid reflux? Do you have a trigger food or drink? How do you deal with it?
When diagnosing diverticulitis, the first thing that doctors usually do is carry out a blood test followed by other tests such as CT scans, X-rays and even ultrasounds.
Full Blood Count
The full blood count can tell doctors a lot about your current health. The number of red blood cells can tell doctors if you’re anaemic and perhaps losing blood. But one of the most important markers in a blood test when trying to check for diverticulitis is the white blood cell count.
White blood cells are a part of the immune system and are responsible for fighting diseases and illnesses. When a pathogen (harmful bacteria or virus) enters the body, it is identified by the immune system which then increases the number of white blood cells. An amount of white blood cells higher than the normal range could be considered to be a sign of infection. However, it is possible to have diverticulitis but not have a measurable increase in white blood cells. So a normal blood result doesn’t necessarily mean that you don’t have an infection or inflammation in the bowel.
CRP (C-Reative Protein)
CRP is known as an inflammation marker – it is a protein released by human tissues when they are inflamed. The higher the amount of CRP in the blood, the more inflammation there is. Having elevated CRP in addition to abdominal pain and other symptoms is a good indicator of diverticulitis. However, your doctor should also check carry out an abdominal examination too just in case the inflammation is coming from somewhere else.
An abdominal exam can help doctors find out if there is anything strange going on…
Abdominal Examination
It’s likely your doctor may carry our an abdominal examination. This is where the doctor will press on your abdomen to discover where the pain originates and if it is the bowel that is inflamed. It’s important to be very honest about the pain you are feeling at this point so that the doctor can rules out any other issues or sources of inflammation.
CT scanner…in you go!
CT scan
This is usually the most effective way to diagnose diverticulitis. A CT scan can be done with or without contrast, but contrast certainly helps when interpreting the results. The two main types of contrast are oral and intravenous (IV). The oral contrast is often a liquid mixed with water that you drink before the scan. It helps to highlight the digestive tract on your scan. The IV contrast is injected into a vein and reaches the tissues and helps them show up better on the scan. Some hospitals may choose to have their patients take both types of contrast. However, it is important than you let the doctor know of any allergies you have before you receive any contrast agents.
A CT scan is painless and just requires the patient to hold their breath for short periods. Let the technician or doctor performing the scan know if you suffer from asthma or COPD or any problem that makes you find it difficult to hold your breath.
After the scan, your results will not be ready immediately since they will need to be looked at by a doctor and a thorough report written. See my post on CT scans for more information.
X-rays
Some doctors may choose to send their patients for X-rays. This is to check for perforations in the bowel since X-rays can easily pick up excess gas in the abdomen that may be leaking out from the bowel. The results of an X-ray are much more immediate which is why this test might be chosen particularly if the patient is in a lot of pain or has a history of perforations and sepsis.
Ultrasound
Again, some doctors may want to send their patients for an ultrasound. This is very common during first time diagnoses when patients are doctors don’t know that the patient even has diverticular disease yet. An ultrasound may also show an abscess or cyst as a result of diverticulitis. It may also be able to detect excess air of material in the abdomen. However, it is not as clear as a CT scan, but the results are more immediate.
Why don’t doctors use colonoscopies to diagnose diverticulitis?
It’s very rare that a doctor would use a colonoscopy to diagnose diverticulitis because while a patient has an infection, it would be very painful and a little dangerous to insert an endoscope. There is a chance that the colonoscopy during an infection could make it even worse or could even cause damage to the colon.
Have you been diagnosed with diverticulitis? Which methods did the doctors use to diagnose you?
So, you’re waiting to get your gallbladder removed – Don’t worry, it’s not as bad as it sounds. In fact you can read about what gallbladder removal surgery entails here or you can read my own story on getting my gallbladder removed.
To avoid extremely painful gallbladder attacks or the worsening of your condition while waiting for your surgery, you can aim to have a low-fat diet. A diet low in fat will hopefully ward off any painful attacks and prevent gallstones from getting larger.
You can eat:
fruit and vegetables
white fish and white meats (no skin and cooked without the addition of fat)
Potatoes (not fried)
2% or less milk and yoghurts
Low-fat cheese such as cottage cheese, feta, etc (check for fat contents of 4% of less)
Try not to do a no-fat diet because this can cause the gallbladder to become even worse. Stick to low-fat and try not to eat large portions. Instead aim to have smaller snacks and portions throughout the day. This will help your gallbladder keep working and prevent discomfort after eating.
Want to know more about what comes next? Read Gallbladder Removal Surgery – Cholescystectomy and let me know what you think.
Gallbladder removal or a cholescystectomy is a common surgery carried out by surgeons all over the world. The gallbladder is an organ located in our upper-right abdomen, just beneath the liver. It is the place where bile is stored. Bile is a yellow/green liquid produced by the liver when it breaks down substances in the body (including our old red blood cells).
The job of bile in the body is to emulsify fats – it does this by breaking up the fats and oils we consume into smaller droplets so that our body can digest it more easily. It also helps to neutralise the acidic chyme (food + stomach acid mixture) that leaves the stomach and enters the small intestine.
The reasons for a cholescystectomy include;
gallstones
gallbladder disease/infection / cholecystitis
non-functional gallbladder/gallbladder sludge
polyps
So what is the surgery like?
Well, these days, most cases are done laparoscopically. This means that it is done using several small incisions in the abdomen (for example in the navel, right side of the abdomen and possibly an incision in the centre of the upper-abdomen. Most patients have three or four incisions, but there are cases of people having less or more. The surgery is carried out under general anaesthetic. This means that you’ll be asleep and unaware of anything going on. Most patients are intubated (with a breathing tube) for this procedure, but are not usually catheterised. The surgery usually lasts between one and two hours. Depending on your hospital, some people may go home the same day and in others, they may be asked to stay in hospital overnight.
If you have an open surgery, the surgeon will make a large incision in the upper-right abdomen and take the gallbladder out from here. This is avoided where possible since it increases the length of time needed for recovery and hospitalisation.
During a laparascopic surgery, the surgeon will inflate the abdomen with gas. This helps provide more space in side to move around and perform the procedure. Then a camera will be inserted into one of the incisions so that the surgeon can see what he is doing. After this, various tools will be inserted into incisions to cut the gallbladder free. Medical titanium surgical clips will be placed to cut off tubes that connected the liver to the gallbladder. These metal clips will remain inside your body for the rest of your life.
Of course like any surgery, it does carry risks and there are complications that can arise. However, for this surgery, complications are rare and most patients deal with it very well.
What is the recovery period like?
Well, for me, it wasn’t too difficult. But everyone heals at different speeds and has a different experience without their gallbladder. Some people are back at work within a few days, and others may take a couple of months to get back to normal.
My advice is not to rush yourself. Recovery is an important process for our body and to recover well you need to rest and relax while trying to stay healthy. Your surgeon will give you some guidelines for aftercare and recovery, so it’s important to stick to those as much as your possibly can.
General guidelines include:
No lifting/carrying for 6 weeks – During the surgery the abdominal muscles are often cut. Heavy lifting, carrying or even straining on the toilet can cause these muscles to separate and increase your risk of a hernia.
No baths – whether your surgeon has used stitches or medical glue, it isn’t advisable to take a bath too early on. The water can soften the healing tissue or the glue and can increase the risk of infection. Taking a shower might be okay, but you should ask your surgeon if they recommend covering the incisions with waterproof dressings beforehand.
Check the incision sites regularly for redness, feeling warm to the touch and weeping. Clear fluid weeping from incisions may be normal, but if the fluid is yellow and opaque and/or you have any of the above symptoms, it may be worth mentioning to your surgeon.
Stick to a post-op gallbladder diet if given one.
Take regular, gentle exercise but DON’T overdo it!
To read about my gallbladder story click here! Want to share your story? Get in touch with me so that we can tell your story, too!
My gallbladder story is quite short really and
uncomplicated in comparison to others. I’d never really experienced any
problems with my gallbladder. Although, looking back, there was a time I had a
sharp and horrendous pain in my upper-right abdomen in 2012 one day while at
work. The pain was severe and my boss called an ambulance which came right away
and injected me with a load of pain killers and muscle relaxants. I went home
and slept it off and the pain was gone within a few hours so I never even went
to a doctor about it. Maybe, that was an attack, maybe not.
Fast-forward to the beginning of February 2019. I was still being investigated after a complicated case of diverticulitis that resulted in the perforation of my bowel and a battle with sepsis. My constant lower-abdominal discomfort caused my gastroenterologist to send me for a full abdominal ultrasound. He wanted to rule out abscesses, cysts and adhesions so requested a scan of the whole abdomen.
Ultrasounds are no big deal. Totally painless and easy to do.
At the ultrasound, the doctor started snapping
pictures of my organs and measuring dimensions, then, the moment he got a clear
image of my gallbladder, he asked ‘Are you on the waiting list to get this
removed?’, ‘No’ I replied, ‘Why do you ask?’ and he told me that there were a
few small stones in there, but more importantly a polyp. I told him I had no
idea and hadn’t had any symptoms of things not working well. Anyway, at the end
of the ultrasound, he gave me all the printed photographs and a written report
detailing what he had found and told me to go back to my gastroenterologist as
soon as possible.
The gastroenterologist told me that it would need to be removed and set up a meeting with a surgeon for a few days later. He looked at my results, agreed that it needed to be removed because of the potential for the polyp because of its size to be a risk. He penciled me in for two weeks later to get it removed. In the mean time, he told me to eat a low fat diet and gave me a list of foods to avoid. (I’ll post about this soon, I promise)
Before I knew it, it was removal day. At 7:30am
I hopped onto the trolley and was taken down to surgery. I watched the staff
running around doing last-minute checks and preparation. It was fun chatting to
the hospital porter who spoke pretty good English and was so smiley. I wasn’t
particularly nervous or scared, I deal with hospital and needles etc pretty
well and I’m not someone to get themselves into a state about a surgery. I’m
sure I was mid-sentence joking with the surgeon and porter as I drifted off
into a deep sleep and the surgery
began.
In what seems like no time at all, I wake up in
a different room with an IV in the opposite arm and a drain coming out of a
hole in my upper-right abdomen. I look to my right and the porter is stood
there smiling. I smile back and say ‘I need to sit up’, He immediately props
the trolley up and hands me a little sick bowl….no, I say, I feel like I can’t
breathe. So, he calls over a nurse who measures my oxygen levels and rushes off
and comes back with a mask. I’m hooked up to oxygen and starting to catch my
breath. Five or ten minutes later, the porter takes me back to the ward where
my boyfriend was waiting to see me. He seemed worried, I asked him what the
problem was and it was only then, that he told me that the surgery was expected
to last maybe an hour and a half, but that I had been there for over four hours
due to it being a tricky surgery. I hadn’t even noticed what the time was.
I expected to be in major pain the rest of the day, but other than a horrible discomfort in my back and shoulders, I had no pain at all. I refused dinner when the nurse brought it. I wasn’t hungry at all and the noodle soup did NOT look appetizing at all. I was alone now because my boyfriend had left for work. I forgot I had the drain and as I got up out of bed and went to the bathroom, I must have moved the drain a little and it was a bit sore. After the effort of that, I went back to bed and was in a little pain. The nurse came to check on me and when I told her it was sore, she injected something into my IV and the pain subsided and I drifted off again.
I woke up the next morning feeling quite chipper. I still had some discomfort in my back and chest from the gas, but was keen to get up and about. I got up had a wash, brushed my teeth and did my hair. Then I got changed. When the nurse offered pain relief via the IV, I declined since I didn’t have any pain except for the gas pains. I got up and walked around the ward and the catering team brought me a chamomile tea which I sipped at.
My surgeon came in to speak to me and told me not to lift heavy things or to strain when going to the bathroom due to the risk of getting a hernia. I was a little worried since I had pushed a bit going to the toilet in the morning, but it was okay, the stitches had held. He removed the drain and replaced my dressings. Before telling me to take almost 3 weeks off work and discharging me from the hospital. He told me to clean my wounds and replace the dressings each day. He also advised me to take a paracetamol if I was uncomfortable, but to contact him if I had severe pain, or jaundice.
I didn’t even need the paracetamol. Recovery wasn’t too difficult, but I stuck to the post-op gallbladder diet that he gave me. (I promise I’ll write about this, too) The one thing I had a problem with, was laying down. The stitches were tight and I couldn’t lay down or get up, so for the first week, I slept sitting up on the couch. It wasn’t a problem.
Sleeping on the couch wasn’t so bad!
I used glycerine suppositories everyday to keep me going to the bathroom without effort. As the days passed, I found doing things even easier and as time passed I found myself able to tolerate more foods. The surgeon checked up on me regularly via telephone and asked me to send him pictures of the healing incisions on Viber. They were all doing great accept for my belly button which was weeping and a little sore and hot to the touch. Although, the surgical incision in my belly button did become a little infected and I had to pack it and take antibiotics, but within a week, it was much better and I could go to have the stitches removed. I had to be careful to stay near a toilet after trying a new food though because a few times in those first couple of months, I experienced dumping syndrome and had to make a bee line for the bathroom.
Post-op, life isn’t much different for me. I sometimes still get dumping syndrome, particularly if I eat something too fatty. Otherwise, I don’t have any real symptoms…just like before my op. However, it’s nice to know that the polyp was removed and won’t be causing any trouble in the future.
So, if you’re having your gallbladder removed. Don’t worry. It isn’t as bad as you might think. If you are suffering with a lot of anxiety, tell your doctor. There are things they can do to help you relax and to reassure you about the surgery. Of course, everyone’s gallbladder story is a little different. But, this is mine and from my experience, I feel it wasn’t a bad or scary experience. But, it is so important to take time out to recover.
My advice is to not push yourself or overdo it during your recovery – you may regret it. Also, don’t expect to feel back to normal immediately. The human body is amazing, but it certainly needs to be given the time to heal after surgery.
If you’ve got diverticular disease (DD)/Diverticulosis, you may be unlucky enough to experience diverticulitis. Don’t know the difference? Check out my post on Diverticular Disease/Diverticulosis Vs Diverticulitis. Diverticulitis is an inflammation or infection of one or more of the diverticula (pouches) in your bowel. Diverticulitis can vary in severity and can go from being a mild flare up, to an infection so severe that it can carry life-threatening complications. So, what can you do if you suspect you may be getting a flare up?
For a start, symptoms of a flare up can include:
abdominal pain/discomfort
high temperature/fever
painful bowel movements
generally feeling poorly (nausea, headache, stomachache)
diarrhoea/constipation
loss of appetite
Change to stools (excessive mucus, blood, huge change is regularity or stool type)
If you are experiencing some of the symptoms above, it’s a good idea to prepare for a flare up by doing the following things:
DO:
drink lots of water – 2-3 litres a day will help flush your system and keep you hydrated. It may also help relieve constipation.
Try a clear liquid diet – eliminating solid foods and dairy from your diet for a day is the best way to rest the bowel and give time for the inflammation to go down on its own.
Keep track of your temperature – on a notepad, note down your temperature every couple of hours so you can monitor any changes. Please note that diverticulitis does NOT always cause high temperature/fever.
Rest – Take time to relax and rest as well as removing yourself as best you can from stressful situations. Sometimes a duvet day and a few extra hours sleep can help the body heal.
Listen to your body – Remember that our body usually knows what is best for it. For example, if you’re tired and want to sleep, do it. If you have no appetite, don’t eat just because it’s dinner time and someone has said you ‘should eat something’.
Take paracetamol-based pain killers to relieve the pain if necessary. This include brands such as Panadol in the UK or Tylenol in the US.
Seek advice from a medical professional – If you are in a lot of pain, have a very high temperature or feel very unwell, it’s a good idea to seek medical advice from a professional. This may include booking an appointment with your GP/PCP, Gastroenterologist/GI doctor or even visiting the local A&E/ER.
If you suspect you may be experiencing a flare up, there are a few things you should avoid doing in order to not make things worse.
DON’T:
eat high-fibre foods – If you suspect a flare up, it’s best to go for a clear liquid diet, but if you want to try solid food, you should stick to low-fibre/low residue foods such as white bread, chicken breast, white pasta or rice.
Take NSAIDs without approval from a medical professional – NSAIDs are not recommended for people with diverticular disease because they can increase the chance of bleeding from the diverticula or increase the risk of perforation.
Take Codeine-based painkillers without approval from a medical professional – codeine is known for causing constipation and so can worsen the infection if stools are not passed through the bowel.
Eat large portions – if you decide to eat, stick to small portions that won’t overwhelm the system.
Take anti-diarrhoea medication without approval from a medical professional – stopping diarrhoea can be a bad thing since you may be keeping infected waste inside your bowel and allowing the infection to become more severe.
These tips and tricks may be able to help you rest the bowel before medical treatment is required. However, if your symptoms become worse or do not subside, it’s important to seek advice from a medical professional.
If it turns out antibiotics are required, there are a number of things you could be prescribed. For example, common antibiotics include: Ciproxin, Flagyl (metro), Co-amoxiclav, Augmentin and several others. However, Ciproxin and Flagyl are the ones most suitable for those with a penicillin allergy. Please note that some of these antibiotics have some significant side-effects and you should make yourself aware of these by reading the leaflet or discussing it with your doctor before you take them.
In a more severe situation, you may even be admitted to hospital to receive treatment for diverticulitis. Here, they will usually give you antibiotics, fluids and pain relief intravenously. You can read about what I like to pack in my hospital bag here.
What symptoms do you experience before a flare up? Have you managed to treat a flare up without antibiotics? How did you do it?
Support the author and buy her a coffee by making a donation here: paypal.me/haylaki
So, you’re going for a colonoscopy…don’t worry. It’s not as bad as you might think! A lot of people say that the preparation is worse than the procedure, so let’s look at how we can make it as smooth a ride as possible.
Two days before the colonoscopy
Reduce the amount of fibre in your diet and adopt a low residue/low fibre diet. Cut out fruit and vegetables and eat plain foods such as chicken without a sauce, white rice, white bread, and clear soups. This makes the preparation much easier on your body. Also eat lightly, try not to eat too much, have small portions and drink lots of water. You may feel quite hungry, but, this will certainly reduce the amount of toilet trips when you take your preparation agent.
Preparation day – On the day before the colonoscopy
I prefer to book a morning appointment for my colonoscopy and not eat anything on the day before my colonoscopy. However, if you have booked a later afternoon or evening appointment, your doctor should give you a schedule for when to take your preparation agent and stop eating and stick to a clear liquid diet.
NOTE: You MUST tell the colonoscopy team or your doctor before doing the preparation if you are diabetic.
When I had my colonoscopy, my doctor gave me Citrafleet to use. It was in two sachets each of which were to be mixed in one glass of water. The Citrafleet tasted like lemon and was definitely fine to drink without too much trouble.
The preparation agent my doctor prescribed for me.
Some doctors give their patients different preparation agents, these can come in large bottles, sachets and some are difficult to drink. Tips for making these drinks more palatable include: keeping it cool, using a straw, adding a flavour or chasing it with a clear drink you enjoy.
REMEMBER: Avoid eating or drinking anything that is red, pink or purple in colour. This can stain the lining of the bowel and can affect the results of the colonoscopy.
Prep day kit!
prep agent
drinks – I had green tea, water, iced tea, Sprite
Vaseline
baby wipes
A show or set of movies that you know well and love to watch.
Someone to hang out with
hobby (crochet, reading, etc)
paint your nails, do a face mask, do your hair, etc.
The urge to go can be sudden and come from nowhere…be ready to spring up and run to the bathroom! Be careful of cables, yarn, being in a position or chair you find it difficult to get out of. Make sure your route to the bathroom remains clear. And that other family members or friends if possible can use a different bathroom if you’ve got your stuff set up in the most convenient one.
Ouch it burns!
Like with any time we get diarrhea, it can burn. So, to solve this, be proactive. Before you go for the first time, apply Vaseline or Sudocrem thickly. This will act as somewhat of a barrier and will protect your skin. Then after going to the bathroom, avoid wiping multiple times with toilet paper. If you suspect it is messy, consider using a bidet or using water to clean your bottom. Alternatively, I would recommend using baby wipes for sensitive skin. These can help you clean up without too much repeated wiping and are gentle on the skin. (the more you wipe over the same area, the more likely it is to become sore). When you’re clean, apply a new thick layer of Vaseline or Sudocrem ready to protect you the next time. This helped me so much!
NOTE: We love the environment so please don’t flush your baby wipes away. Of course it would be better not to use them at all, but it’s better to dispose of them in a bin rather than flushing them down the toilet where they can block drains or enter our waterways.
How do I know whether I’m empty and ready for the procedure?
In theory, by the end of the preparation, your bowel movements should be totally liquid, pretty much see-through and possibly yellow in colour. If you are still passing loose stool with pieces in it or thick and not at all see-through, you should contact your doctor or a member of staff at the place where the colonoscopy is taking place. Some places will do an enema if the bowel requires a little cleaning, but others would rather reschedule the colonoscopy and prescribe a different preparation agent.
Good luck for the procedure!
If you have any more questions about preparing for a colonoscopy, please ask them in the comments below and I’ll try to answer them or even add additional information to the blog post. How did your colonoscopy prep go and do you have any helpful tips?
Maybe it’s just me, but after being in hospital a few times with diverticulitis and then from a gallbladder removal surgery, I like to make sure I always have a bag ready for the hospital. Usually, this bag lives under the bed, but sometimes it accompanies us in the back of the car on long journeys and trips. But, it makes me feel better knowing that everything I need is ready to grab and go should I end up in hospital. Below, I’ve included my list of things that I keep packed in my hospital bag.
My List
pyjamas/nightie
comfortable and easy to put on footwear (e.g. slippers/sliders/crocs/flip flops)
underwear
wet wipes
toothbrush/toothpaste
hairbrush and headbands/hair ties
lip balm
flannel/face wash cloth
travel soap/liquid soap/body wash
towel (not white)
pillow (not in a white pillow case)
chargers for any smartphones, tablets, e-readers
feminine hygiene/sanitary products
comfortable bra/bandeau bra
If course, if it is a planned visit, you can pack especially for your stay remembering to include any books/tablets/chargers/etc. medications.
If you don’t want to have a bag packed constantly, I’d recommend keeping a list of everything you’d like to have with you in the hospital so that if the worst happens, either you, a family member or a friend can see exactly what to pack for you – and do it relatively stress-free. You can keep the list stuck to the fridge or family notice board or even inside the bag or suitcase you would use to pack for the hospital so that it’s in there for when you need it.
What do you think of my hospital bag list? Is there anything else you always take with you? Let me know in the comments.
Keeping a
diary isn’t always easy, but…it can come in very handy, especially if you are
still learning to manage a health condition. If you are someone that already
keeps a daily diary or journal, it may be easy to add this information in to
your entries. However, if you’re not someone used to keeping a diary, then you
can find other ways to do it, for example, you can use the downloadable
attachment here, and complete that each day before filing it away, or you can
create your own version that applies more specifically for you. Not only will
this help you identify trigger foods or patterns in your symptoms but it could
also be a great tool to help your doctors monitor and manage your health.
NOTES:
Be honest! Write what you really ate and drank….snacks, junk and alcohol included…you need to see the whole picture, exactly as it is.
Take it to
doctor’s appointments with you even if you don’t need to use it. You never know
when the info could come in handy.
If you have
a bullet journal, you can get really creative with this. I’ve given you guys a
free downloadable and printable version of what I use. Now, unfortunately you
do need to print it to get the best use out of it. I would recommend filing
them each day in a binder to keep a continuous diary. How much additional
information you record is totally up to you. However women may benefit also by
tracking their menstrual cycle, too.
DD Tracker Printable
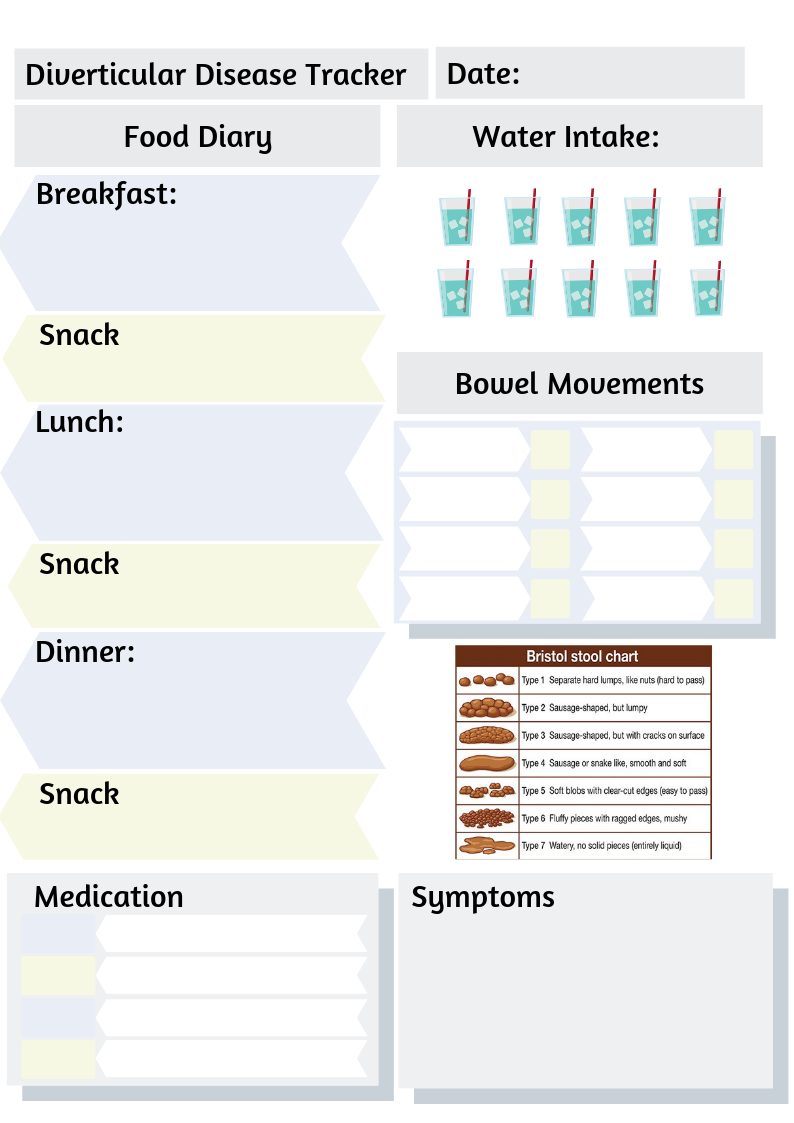
I’ve put together a little Diverticular Disease/Diverticulosis Tracker. You can use this to monitor what you eat, how you feel and even keep tabs on your bowel movements. I hope this proves to be helpful. The file even has it’s very own instructions that show you exactly how to use it. Just click on the download button below for FREE and you can print it out right away. Support the creator and buy her a coffee by making a donation here: paypal.me/haylaki
Food Diary: The food sections allow space for you to write about what you ate and drank for the day.
Water Intake: You can cross out or tick the glass of water to show how much you drink each day.
Bowel Movements: The stool section provides boxes for you to keep a record of your bowel movements. There is space to write a time and or comment and a number that corresponds to the Bristol stool chart.
Symptoms/other notes: here you can mention any other feelings or symptoms you experience even if you feel they aren’t relevant. For example, headache, joint pain, nausea, delicate mood, etc. or even record that you took pain medication or anything that you don’t usually take. In addition, you could note anything else there you wish.
Medication: It’s always worth making a note of any medication you had to take, whether it seems related or not. But taking medication such as painkillers or antacids is a good way to keep a record of how often your symptoms bother you enough to reach for the medicine cupboard.
Tracker Previews
Preview of the DD Tracker Instuctions and examples
Let me know what you think and even share with me what you record in your diary to help you…do you do anything differently?